
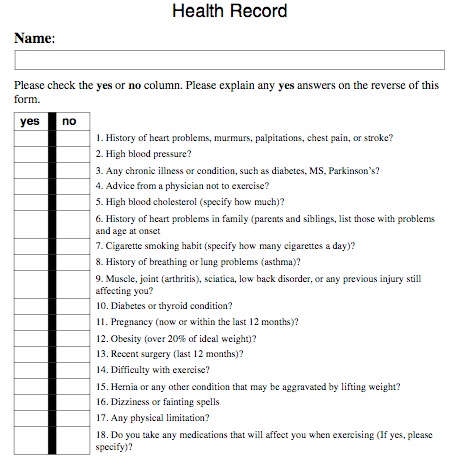
Health Record and Release
All who participate in any of the AFTA evaluation must fill out and sign AFTA’s health
record and testing release form.
Make sure your clients or yourself have no more than 1 coronary risk factor as well as being absent of
disease or orthopedic problems that would prevent them from exercising. Make sure all
clients or yourself are healthy and able to undergo the rigors of testing. If you think they are at risk or yourself, please get a doctor’s note before testing. Record any pertinent medical information on
AFTA’s health record.
•Coronary risk factors – age, hypertension, blood cholesterol, smoking, diabetes, family
history of heart disease.
•Disease – asthma, diabetes, MS, Lupus, Parkinson, diabetes, heart disease, and others.
•Orthopedic – current or previous broken bones, sciatica, shoulder impingement, includ-
ing rotator cuff problems, and knee, hip, and low back pain, and others.
Go over their or yourself current, as well as previous activity history, and record all pertinent informa-
tion. In addition, you must have them fill out or yourself a release section stating that you’re not lia-
ble, that they are freely volunteering to be tested, and that they are free of medical
problems. Explain to them and understand yourself the rigors of undergoing testing and that they or
yourself will feel sore the next day. Also, they or yourself should only push themselves or yourself to a point they can tolerate and not to a point where injury may occur. You must not push a client or yourself beyond their or your ability and experience.
Physician clearance before testing is recommended at or above the age of 40 in men and
50 in women. Physician clearance before testing is also recommended in individuals with
two or more coronary risk factors and/or symptoms of cardiopulmonary disease, chronic
orthopedic problems, and disease. Physician clearance is recommended in any case where
you think there may be a problem.
Physical Fitness Testing Consent
Objectives
I understand that the tests that are about to be administered to me are for the purpose of determining my physical status, which may
include heart, lung, and blood vessel capacities for whole body activity, body composition (ratio of body fat to muscle, bone, and
water), muscular endurance and strength, and joint flexibility.
Explanation of Procedures
I understand that the tests that I will undergo may be performed on a treadmill, bicycle, or steps. The tests are designed to increase the
demands on the heart, lung, and blood vessel system. This increase in effort will continue until semi-exhaustion or other symptoms pro-
hibit further exercise. During the test, heart rate will be periodically measured. Body composition will be determined through use of
skinfolds and tape measure to determine levels of body fat versus fat-free weight. Some parts of the body needs to be exposed and
pinched with a caliper and measured with tape. Muscular endurance and strength will be determined through use of body calisthenics
and/or equipment. The sit-and-reach test and other stretch tests will be used to determine flexibility.
Description of Potential Risks
I understand that there exists the possibility that certain abnormal changes may occur during the testing. These changes could include
abnormal heart beats, abnormal blood pressure, various muscle and joint strains or injuries, and in rare instances, heart attack. Profes-
sional care throughout the entire testing process should provide appropriate precaution against such problems.
Benefits To Be Expected
I understand that the results of these tests will aid in determining my physical fitness status, and determining potential health hazards.
These results will facilitate a better individualized fitness analysis.
Physician Consent
Physician clearance is recommended at or above the age of 40 in men and 50 in women before testing. Physician clearance before test-
ing is also recommended in individuals with two or more coronary risk factors and/or symptoms of cardiopulmonary disease, chronic
orthopedic problems, and disease. Physician clearance is recommended in any case where you think there may be a problem.
Signature
I have read the foregoing information and understand it. Questions concerning these procedures have been answered to my satisfaction.
I also understand that I am free to deny answering any questions during the evaluation process or to withdraw consent and discontinue
participating in any procedures. I have also been informed that the information collected is confidential and will not be disclosed to any-
one other than my physician or others who are involved in my care or exercise prescription without my permission (see permission to
disclose information). however, I am in agreement that the information from these tests not be identifiable to me can be used for
research purposes. Please sign and date.
PARTICIPANT:
DATE: